2025 Fentanyl Report
2025 Fentanyl Report
Overdose Response Strategy | Public Health/Public Safety Partnership
SIAC Product: 250707-1321220
Release Date: 07/10/2025
In partnership with:
- Utah Department of Public Safety
- Utah Poison Control Center
- Overdose Response Strategy (ORS)
- HIDTA / CDC Foundation
- Utah Department of Health & Human Services
Disclaimer: "This project was supported by Grant No. 2018-PM-BX-K021 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance is a component of the Department of Justice's Office of Justice Programs, which also includes the Bureau of Justice Statistics, the National Institute of Justice, the Office of Juvenile Justice and Delinquency Prevention, the Office for Victims of Crime, and the SMART Office. Points of view or opinions in this document are those of the author and do not necessarily represent the official position or policies of the U.S. Department of Justice."
This report was supported in-part by the Centers for Disease Control and Prevention (CDC) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $17,000,000, with 100 percent funded by CDC/HHS. A portion of this funding supported the project described above. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement by, CDC/HHS, the U.S. Government, or the CDC Foundation.
Executive Summary
This report investigates the evolving nature of drug use, now primarily supply-driven, rather than demand-driven. Illicit drug manufacturers have gained power through producing drugs more efficiently and at lower costs. With low cost operations, illicit drug manufacturers have been able to traffic more drugs through supply chains than in previous years. Due to its high volume production, illicitly manufactured fentanyl (IMF) has flooded U.S. drug supply, amplifying addiction in people who use drugs. Evidence shows that during the peak of first-fentanyl use (2012-2014), people who used drugs preferred not to have fentanyl in their supply as it was an unknown substance with a high potency.
Today, fentanyl has ushered in a "fourth wave" of the drug epidemic, known as polysubstance use, leaving many Utahns to assume fentanyl is normally present in their drug supply. Across the United States, the use of IMF has drastically increased, resulting in more accidental overdoses. The United States has responded to this tragedy through targeted evidence-based harm reduction methods, and Utah has made major strides in helping people who use drugs find treatment and low-cost resources to aid them on their journey to recovery.
However, a noticeable shift in 2022 to 2023 occurred when services offered by harm reduction programs decreased, and all drug overdose deaths in Utah increased by 12%. The following year (2023 to 2024), the reverse occurred, where services provided by these programs increased in participation, and all drug overdose deaths decreased by 2.5%*. Though participation in harm reduction programs varies year to year, it is evident that these groups provide key services, and disruptions to their programming can play a significant role in the number of drug overdose deaths in Utah.
The Utah Drug Monitoring Initiative, in collaboration with the Utah Statewide Information & Analysis Center (SIAC) and the Utah Fentanyl Task Force, organized and coordinated an expert evaluation to estimate the progress made in Utah on recommendations made by the 2021 fentanyl report. Those estimations led to a list of ten new recommendations for the reader to consider. A summary of those recommendations can be found on page 20 of this report with detailed commentary following.
Introduction
In 2021, the Utah Drug Monitoring Initiative published its first fentanyl report, offering an in-depth look at the rapid growth of illicit fentanyl use in Utah and across the United States. This 2025 report is a continuation of the 2021 report providing updates to the fentanyl crisis in Utah. This report aims to acknowledge the many local partners who have contributed to this report and to the many efforts taking place throughout the community to reduce overdose fatalities.
Though this report looks deeper into the fentanyl crisis in Utah, in terms of use patterns, seizures and fatalities, it is important to consider the social and structural levels of risks many people who use drugs (PWUD) encounter which this report cannot thoroughly examine. Social determinants of health, or root causes, contribute significantly to a range of drug use events including first use and fatality. These root causes include, but are not limited to, (1):
- unstable housing,
- economic stagnation,
- class-based despair (i.e. economic hardship, social isolation, loss of meaning),
- geographic heterogeneity (especially seen in rural areas),
- employment history,
- incarceration and criminal history (both individual and family),
- inequitable access to healthcare
Geography plays a significant role in Utah's overdose epidemic with supply and demand forces rapidly being influenced by supply variations across the U.S. to state-level street marketing strategies. This report dives deeper into the use of illicitly manufactured fentanyl (IMF) both in Utah and through seizure data, forensic and toxicology data as well as surveillance data.
What is Fentanyl?
It is commonly known that fentanyl is a synthetic opioid drug that was first introduced in the 1960s as an intravenous anesthetic. It is approximately 100 times more potent than morphine and 50 times more potent than heroin. Fentanyl is a highly potent compound that bonds strongly and preferentially with opioid receptors in the brain. Once bonded with these receptors, fentanyl causes analgesia and stimulates areas of the brain responsible for addiction (2). Along with analgesia, fentanyl commonly causes relaxation, euphoria, sedation, confusion, drowsiness, dizziness, nausea, vomiting, urinary retention, pupillary constriction and respiratory depression (3).
Fentanyl is a Schedule II narcotic under the United States Controlled Substances Act of 1970. Fentanyl is defined as a "drug with high potential for abuse, with use potentially leading to severe psychological or physical dependence (4)." A summary of the federal trafficking penalties for fentanyl and fentanyl analogues can be found in Table 1.
Throughout the U.S., illicit fentanyl use has been on the rise since 2011 when it was discovered that its manufacturing was associated with drug cartels, alongside fraudulent prescriptions, illicit patient-to-patient and/or physician sharing and theft.


| FEDERAL TRAFFICKING PENALTIES | ||||
|---|---|---|---|---|
| DRUG | QUANTITY | PENALTIES | QUANTITY | PENALTIES |
| Fentanyl (Schedule II) |
40–399 grams mixture |
First Offense: Not less than 5 yrs, and not more than 40 yrs. If death or serious injury, not less than 20 or more than life. Fine of not more than $5 million if an individual, $25 million if not an individual. Second Offense: Not less than 10 yrs, and not more than life. If death or serious injury, life imprisonment. Fine of not more than $8 million if an individual, $50 million if not an individual. |
400 grams or more mixture |
First Offense: Not less than 10 yrs, and not more than life. If death or serious injury, not less than 20 or more than life. Fine of not more than $10 million if an individual, $50 million if not an individual. Second Offense: Not less than 15 yrs, and not more than life. If death or serious injury, life imprisonment. Fine of not more than $20 million if an individual, $75 million if not an individual. 2 or More Prior Offenses: Not less than 25 years. Fine of not more than $20 million if an individual, $75 million if not an individual. |
| Fentanyl Analogue (Schedule I) |
10–99 grams mixture | 100 grams or more mixture | ||
Repeated and Chronic Use of Fentanyl
Preclinical and clinical studies show that repeated use of analgesic opioid drugs, including fentanyl, lead to a higher risk of immunosuppression, which is especially dangerous for the elderly and those who are immunocompromised (5). Respiratory depression is the most dangerous side effect of fentanyl use and without monitoring, this reaction could lead to death. Respiratory depression has a five-minute peak after fentanyl has been administered and requires four hours to recover in humans, this high potency drug administration requires appropriate monitoring to gain a full recovery (6).
The growing concern with fentanyl is that, due to its high potential for addiction and misuse, fentanyl has been widely used outside of physician monitoring and its prolonged apnea results in sudden death. In fact, adverse-event reporting systems across the United States, Europe and the United Kingdom have all shown a significant increase of fentanyl misuse leading to increased patient dependence, prolonged hospitalization and death (7).
Fentanyl-Related Overdoses and Fatalities
IMF is illicitly manufactured in cartel laboratories most commonly in pill form or as powder. Due to its low manufacturing costs, fentanyl powder can be readily mixed with one or more drugs to either mimic another drug or to create a more desirable product. Moreover, many people using drugs prefer not to use fentanyl and may be unaware of having taken it at all. Due to its odorless and tasteless character, fentanyl can be added to other drugs leaving the person completely unaware of its presence. In British Columbia, a study conducted in 2015 showed that 29% of the drug screens performed at 17 different harm reduction sites showed the presence of fentanyl; 73% of those reported they did not know that fentanyl was present in their supply (5).
Though the reason drug cartels insert fentanyl powder into their products cannot be conclusively determined, it is known that the significant increase in illicit manufacturing of fentanyl and fentanyl analogs mirrors the significant rise in drug overdose deaths related to fentanyl (9).
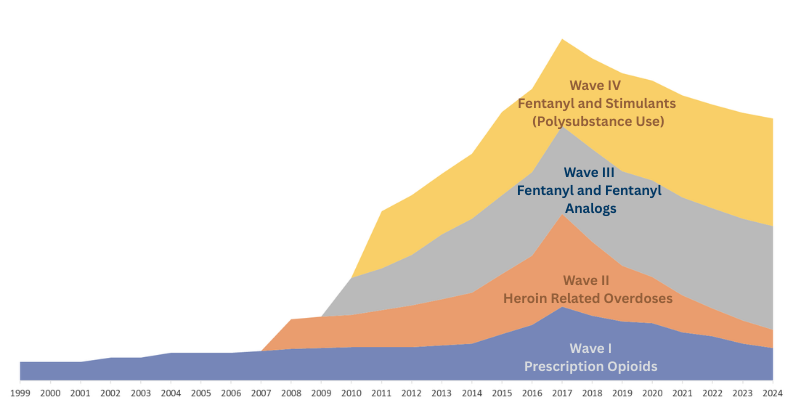
The Overdose Epidemic and Wave IV
Across the U.S., the overdose epidemic is described as a quadruple wave phenomenon (10). Wave I emerged in the early 2000's with fatal drug overdoses dominated by prescription opioids, seeing a sharp rise in 2017. Wave II emerged as heroin-related overdoses surged around 2010, peaking in 2017. Wave III is defined as the onset of fentanyl and fentanyl analogs. Evidence does show; however, fentanyl was detected prior to the onset of Wave III but was generally mimicking heroin and sold as heroin (11).
Currently, the U.S. is in Wave IV: stimulants and polysubstance use. Wave IV exhibits a sudden shock to the overdose epidemic which is driven by fentanyl and fentanyl analogs in combination with stimulants, resulting in polysubstance use. Though it is complex to understand the pattern of polysubstance use, public safety seizure data and drug trafficking organizations analysis show that polysubstance use is more supply-driven rather than demand-driven (12). This trend is especially concerning as PWUD have reported a preference to not use fentanyl but are typically unaware of the presence of fentanyl in their supply (unpublished data).
Fentanyl and Fentanyl Analogs
The supply, distribution and potency of IMFs continues to be a growing concern across the U.S. In 2017, The U.S. Drug Enforcement Administration's National Forensic Laboratory Information System (NFLIS) began seeing an alarming increase in submissions of U-47700, carfentanil (100 times more potent than fentanyl) and 3-methylfentanyl (4 times more potent than fentanyl). During the peak of Wave III of the overdose epidemic, the U.S. experienced a noticeable increase of fentanyl analogs contributing to opioid overdose deaths. In 2016, this trend accounted for nearly half of the opioid overdose deaths (14). An annual report produced by the DEA laboratory offers a snapshot of the increase in new substances seized and analyzed at DEA (annual reports can be found starting in 2016 through DEA's Emerging Threat Reports). In 2016, U-47700, furanyl fentanyl and 3-methylfentanyl were identified for the first time. In 2022, phenethyl 4-ANPP was reported for the first time (15).


Carfentanil and nitazenes are both synthetic opioids known to be extremely more potent than fentanyl. Carfentanil is a commonly used veterinary tranquilizing agent for large animals; however, carfentanil has been detected in DEA drug seizures, including seizures in Utah.
Nitazenes are a group of opioids developed for pharmaceutical research but were not approved for use in the U.S. However, nitazenes slid into the illicit market by way of chemical suppliers who found new chemical combinations to old chemicals which became regulated due to their illicit use. Nitazenes such as isotonitazene, metonitazene and protonitazene are among the most commonly detected nitazenes in polydrug mixtures.
Though carfentanil and nitazene use is periodical, their increased potency can cause a surge in drug overdoses among PWUD. SUDORS data shows an increase in nitazene deaths from 27 in 2020 to 320 in 2023. Carfentanil was detected in a record 277 drug overdose deaths in the U.S. in 2020 which dropped to as low as 7 in 2022, then increased to 168 in 2023.
Both carfentanil and nitazenes are not commonly involved in overdose deaths. Carfentanil was present in five deaths between 2017 and 2018 in Utah and fewer than five deaths in 2024. Though found in drug overdose deaths worldwide, nitazenes were found in only six deaths since 2023 in Utah.


Emerging Threats: Xylazine
Xylazine, also known as "tranq," is an approved sedative and analgesic for veterinary use only. Xylazine is available in a solid form (coming from China and other countries) or in liquid form (believed to be diverted from approved veterinary use). In 2018, xylazine rapidly spread across the eastern states of the U.S., resulting in 102 overdose deaths. In 2021, overdose deaths with xylazine rose to 3,468 with nearly all cases involving fentanyl (16). In late 2022, the U.S. Federal Government confirmed the increasing threat of xylazine in the drug supply and declared it a national threat due to its presence in fatal overdoses.
The rate of xylazine present in the drug supply across the U.S. was relatively low in 2019; however, in 2022 all but two states had reported some level of xylazine. The highest rates of xylazine present in the drug supply dominated the eastern U.S., with the highest rates present in New Jersey, Rhode Island and Maryland (rates reported by DEA NFLIS, 15).
As with many of the fentanyl analogs, xylazine-involved overdose deaths are uncommon in Utah. However, since 2014, ten fatal overdose deaths involving xylazine occurred in Utah, nine of these occurred since 2022 and six between 2023 and 2024.
Utah Crime Lab Submissions
In 2024, approximately 92% of fentanyl samples submitted to the Utah Bureau of Forensic Services (UBFS) by law enforcement agencies were in the form of counterfeit pills or tablets. Most commonly, the counterfeit pills appear similar to pharmaceutically manufactured 30-milligram oxycodone tablets. Typically, less than 5% of fentanyl samples were in the form of powder. In 2022, fentanyl was ranked as fourth most common substance found in all submissions to UBFS. Since 2023, fentanyl has become the most common substance present in UBFS samples.
UBFS has seen indications of xylazine in fentanyl exhibits occasionally since 2018; however, it has not been identified by the UBFS for seized drug submissions. UBFS does confirmation testing for controlled substances and xylazine is not a controlled substance in Utah.
| Rank | 2022 Substance | % | 2023 Substance | % | 2024 Substance | % |
|---|---|---|---|---|---|---|
| 1 | Methamphetamine | 28.7 | Fentanyl | 22.5 | Fentanyl | 31.8 |
| 2 | Heroin | 14.6 | Methamphetamine | 21.2 | Methamphetamine | 17.1 |
| 3 | No controlled substances | 10.5 | Heroin | 11.2 | No controlled substances | 9.3 |
| 4 | Fentanyl | 10.4 | No controlled substances | 9.6 | delta-9-THC | 8.4 |
| 5 | delta-9-THC | 9.1 | delta-9-THC | 8.7 | Cocaine | 5.0 |
| 6 | Psilocyn | 4.1 | Cocaine | 7.0 | Buprenorphine (Rx) | 4.1 |
| 7 | Cocaine | 2.8 | Psilocyn | 3.7 | Psilocyn | 4.1 |
| 8 | Marijuana | 2.7 | Buprenorphine (Rx) | 2.7 | Heroin | 3.8 |
| 9 | para-Fluorofentanyl | 2.2 | Marijuana | 1.8 | para-Fluorofentanyl | 3.4 |
| 10 | Buprenorphine | 1.6 | Alprazolam (Rx) | 1.3 | Marijuana | 1.9 |
*UBFS Marijuana leaf technician program eliminates most of the marijuana submissions to the laboratory.
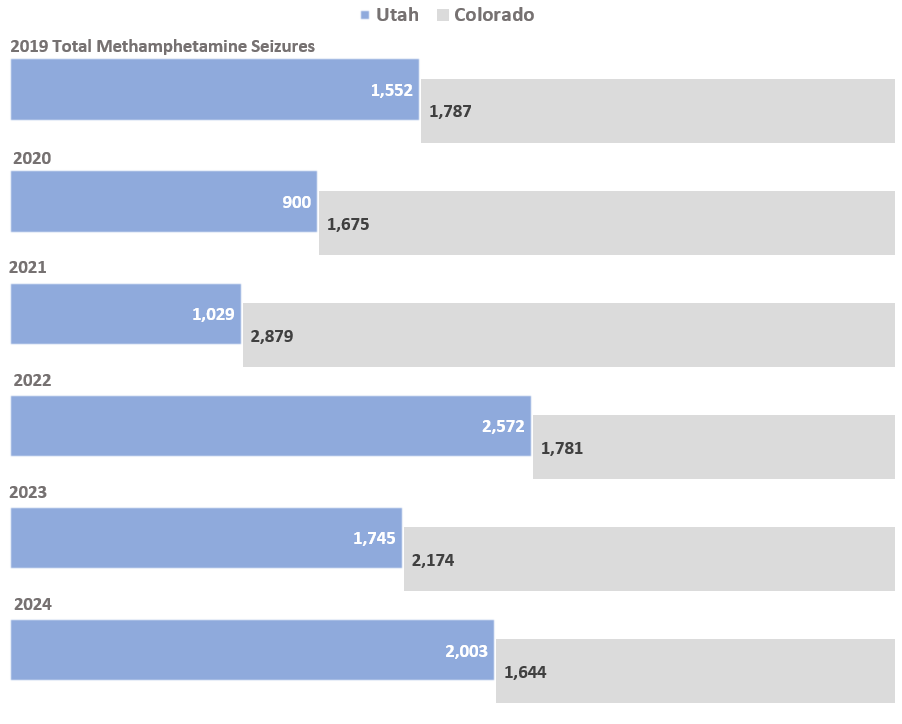
Drug Seizures
Drug seizure data is collected by the Rocky Mountain High Intensity Drug Trafficking Areas (RMHIDTA) for all four Rocky Mountain states (Utah, Wyoming, Montana and Colorado). Displayed here are comparisons of Utah drug seizures to Colorado drug seizures for fentanyl (dosage units and pounds), heroin, methamphetamine and cocaine. Colorado is used as a comparison because of its geographical similarities to Utah and relatively close distance to the U.S. southern border. The flow of these substances over the last five years has increased significantly. From 2019 to 2024, the total seizures of fentanyl in dosage units grew by a factor of 125 in Utah; for fentanyl in pounds, seizure totals grew by a factor of 186.



Fentanyl-Related Deaths Across the U.S.




Today, most fatal overdose cases are a result of polysubstance use, the intentional or unintentional use of more than one lethal substance. SUDORS data since 2020 indicates the five most frequently occurring opioids and stimulants (alone or in combination) involved in overdose deaths across the U.S. From 2020 to 2023, IMFs, used alone, were involved in about a quarter of all drug-related deaths. However, as the presence of IMFs used alone slightly decreased, drug-related deaths using IMFs in combination with cocaine and/or methamphetamine grew across the U.S.
Fentanyl-Related Deaths in Utah
Similar to trends across the U.S., Utah has seen a change in common types of drugs involved in a fatal overdose. Fentanyl is involved in nearly half of all drug overdose deaths. Table 3 displays the top ten list of most common substances found in drug overdose deaths in Utah for years 2022 through 2024, confirmed through postmortem toxicology testing. As fentanyl presence is growing (from 35% in 2022 to 43% in 2024), it is commonly used in combination with other substances. Though fentanyl surpassed methamphetamine in 2023, both substances have historically been the top two substances found in drug overdose cases.
| Rank | 2022 Substance | % | 2023 Substance | % | 2024 Substance | % |
|---|---|---|---|---|---|---|
| 1 | Methamphetamine | 50 | Fentanyl | 48 | Methamphetamine | 44 |
| 2 | Fentanyl | 35 | Methamphetamine | 46 | Fentanyl | 43 |
| 3 | Heroin | 23 | Gabapentin | 17 | Gabapentin | 15 |
| 4 | Oxycodone | 16 | Ethanol | 14 | Ethanol | 14 |
| 5 | Gabapentin | 14 | Alprazolam | 11 | Oxycodone | 11 |
| 6 | Alprazolam | 11 | Oxycodone | 11 | Alprazolam | 11 |
| 7 | Ethanol | 10 | Cocaine | 10 | Cocaine | 10 |
| 8 | Diphenhydramine | 9 | Heroin | 10 | Heroin | 7 |
| 9 | Cocaine | 8 | Kratom | 7 | Clonazepam | 7 |
| 10 | Clonazepam | 8 | Clonazepam | 6 | Methadone | 6 |
Methamphetamine and fentanyl continue to be the most common substances involved in overdose deaths in Utah. In 2024, methamphetamine was involved in 44% of all overdose deaths, followed closely by fentanyl at 43%. The number of heroin-related overdose deaths has steadily declined—from 140 in 2020 to 45 in 2024. Similarly, overdoses involving at least one prescription opioid have dropped from 190 in 2020 to 157 in 2024.
Fentanyl surpassed methamphetamine in 2023 in Utah as the most commonly involved drug in overdoses. Overall, preliminary data from the Utah Office of the Medical Examiner shows a 2.5% decrease in the number of drug overdose deaths in 2024 compared with 2023.

Nearly all local health districts in Utah have experienced considerable increases in fentanyl overdose deaths. It's difficult to interpret changes over time due to small counts but the biggest percent increase occurred in Central, Salt Lake and Southwest Health Districts between 2019 and 2024. The highest rate of fentanyl overdose between 2020 and 2024 was in Salt Lake County, TriCounty and Weber-Morgan health districts. The highest rate of fentanyl overdose across the reporting period was in TriCounty in 2021 and 2023: 15.9 and 15.6, respectively (both of these rates are technically considered unstable as they have a relative standard error higher than 30%).

Users should interpret with caution: rates have a relative standard error greater than 30% and are considered unstable. Wasatch and San Juan health departments have been removed due to small counts.
Surveillance Data: All Drug Overdose Emergency Department Visits
Syndromic surveillance data for all drug overdoses captured by emergency departments (ED) from 2019 to 2024 are displayed below. Syndromic surveillance data provides near real-time reporting of symptoms and syndromes through ED visits; however, this data is subject to limitations that should be considered when interpreting these data (i.e. chief complaint variability, coding delays and errors, data volume and quality, etc). ED data is retrieved through the Electronic Surveillance System for the Early Notification of Community-based Epidemics (ESSENCE) and the rate is calculated for all ED visits for drug-related overdoses (numerator) to all chief complaints in the ED (denominator).
Between 2019-2022, the rate per 100,000 has increased steadily for each Utah local health department region. In 2023, all regions except for TriCounty, showed a slight decrease in the rate of all-drug overdoses. In 2024, all Utah regions showed a decrease in the rate of all-drug overdose ED visits. Tricounty and Southwest have the highest rates of all-drug overdose ED visits since 2019.
| Health Department | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 |
|---|---|---|---|---|---|---|
| Bear River | 95.2 | 82.1 | 162.7 | 250.7 | 226.3 | 212.1 |
| Central | 150.5 | 123.4 | 239.0 | 243.0 | 241.6 | 200.2 |
| Davis | 144.4 | 126.5 | 157.5 | 175.0 | 170.2 | 143.8 |
| Salt Lake | 174.3 | 140.6 | 170.8 | 191.1 | 173.6 | 146.1 |
| San Juan | 131.4 | 154.6 | 232.2 | 83.0 | 59.6 | 26.8 |
| Southeast | 826.4 | 567.1 | 575.2 | 657.9 | 557.2 | 532.9 |
| Southwest | 160.2 | 152.2 | 200.8 | 221.0 | 211.1 | 165.3 |
| Summit | 72.9 | 38.1 | 58.8 | 95.5 | 72.5 | 64.6 |
| Tooele | 264.6 | 176.5 | 152.3 | 184.8 | 160.8 | 144.3 |
| TriCounty | 600.4 | 577.5 | 658.1 | 642.6 | 693.1 | 520.7 |
| Utah | 196.1 | 154.5 | 225.1 | 275.1 | 252.5 | 226.5 |
| Wasatch | 129.2 | 81.1 | 116.9 | 161.4 | 151.2 | 142.6 |
| Weber-Morgan | 220.7 | 164.0 | 217.1 | 229.4 | 217.2 | 169.3 |






Surveillance Data: Utah Poison Control Center
The Utah Poison Control Center (UPCC) provides 24-hour information and education for the state of Utah through phone support for poisonings, including drug-related poisonings. The UPCC first encountered fentanyl in 2020 when patients called in to report an unexpected overdose. The patients believed they were using oxycodone 30mg tablets; however, testing confirmed the tablets were fentanyl with no oxycodone present.
Cases like this were noticed across the U.S. By 2021, this increase was so widespread that poison centers across the U.S. began developing specific codes for the National Poison Data System in 2021 to identify illicit fentanyl use separate from prescription fentanyl use.
As fentanyl cases grew around the country, so did rates in Utah with a large UPCC increase occurring in 2022. Most cases (75%) are related to fentanyl misuse with other reasons including suicide attempt (9%), fentanyl withdrawal (3%), pediatric cases (3.5%) or other situations (9.5%).
UPCC is a distinctive and indispensable resource for the state of Utah, providing a free and confidential phone service to those encountering a poisoning crisis. UPCC has responded to Utah's fentanyl crisis by establishing internal protocol to better assist in fentanyl overdoses and withdrawals. They also provide naloxone training for free; nearly 5000 people have completed naloxone training through UPCC.

Utah Harm Reduction
The Utah Syringe Exchange Network (USEN) is a coalition of over 30 community-based organizations, local governments and other stakeholders working together to provide evidence-based harm reduction services for PWUD in Utah. The Utah Syringe Exchange Network (USEN) comprises state and local agencies, nonprofits agencies, healthcare organizations and concerned individuals working together to bring about healthier communities by reducing the spread of disease and other health concerns among PWUD. USEN is facilitated through the Violence and Injury Prevention program at the Utah Department of Health and Human Services (DHHS).
The mission of USEN is to reduce harm associated with substance use by promoting resourceful and supportive solutions for individuals and communities. USEN works toward this goal by advocating for public health and policy reforms, educating stakeholders, and fostering relationships that bring about opportunities to broaden the reach of syringe exchange programs across the state. Some programs offer unique resources like food banks, clothing banks, and harm reduction-driven support groups. By offering services like these, syringe service programs are able to gain and maintain trust and sincerity with their clients. For many PWUD, this relationship between the client and their syringe service provider (SSP) is crucial for finding treatment and resources to reduce harms from drug use.Utah law requires syringe exchange programs to make available to syringe exchange clients verbal and written instruction on: (1) methods for preventing the transmission of bloodborne pathogens, such as HIV and hepatitis C; (2) information and referral to drug and alcohol treatment; (3) information and referral to HIV and HCV testing; and (4) how and where to obtain an opiate antagonist.
From year 2022 to 2023, SSPs exhibited a decrease in services provided to their clients. The number of naloxone kits distributed to SSPs by the state decreased (-42%) as well as the number of clients served (-18%), the number of new clients enrolled (-26%) and referrals to treatment (-13%). As clients received fewer of these services by SSPs, there was an increase in all drug overdose deaths in the same period (+12%). Interestingly, the reverse was observed from 2023 to 2024 where services provided to clients by SSPs saw an increase and all drug overdose deaths decreased by 2.5%. Figures 11 and 12 demonstrate this shift in participation and services provided, year over year.


2024 All drug overdose death data is preliminary as of May 26, 2025.
Utah Fentanyl Task Force: Recommendations
These recommendations, developed jointly by the Drug Monitoring Initiative and the Utah Fentanyl Task Force, reflect input from local, state, and nonprofit partners involved in illicit drug-related operations. The information provided does not represent the official position of any single government organization.
In 2021 the Utah Drug Monitoring Initiative published the Utah Fentanyl Report, which documented the need for change and ten recommendations to address growing concerns. At the establishment of the Utah Fentanyl Task Force in late 2024, progress regarding the 2021 recommendations was unknown. Leaders of the Task Force's Prevention, Treatment, and Recovery Work Group recognized the need for a baseline measurement to compare subsequent interventions and policy outcomes. In March 2025, this work group invited 45 stakeholders from across Utah to evaluate progression on the 2021 recommendations.
The evaluation asked respondents to reflect on Utah's policies and programs that have contributed to the reduction of fentanyl use, overdose, and fatalities through an online evaluation. Additionally, the Department of Public Safety hosted an in-person event where the evaluation was discussed and new recommendations were reviewed.
The survey asked participants to rate progression in implementation, impact, and access to resources for each of the ten 2021 recommendations with a rating system ranging from very low (1) to very high (5). Experts also had the opportunity to share examples, evidence, and new recommendations. The following tables demonstrate the results including a calculated total of the online and in-person evaluation. Moreover, recommendations listed in this section also include a "Local Efforts" portion in which the Prevention, Treatment, and Recovery Workgroup compared resulting recommendations with similar efforts from the Utah Overdose Fatality Review Committee, TriCounty Health Department and the Utah County Health Department.
Summary of New Recommendations for Utah
- Provide funding for local health departments to utilize public awareness campaigns which promote positive messaging, concentrate messaging to high-risk areas, and encourage the public to seek substance use treatment (i.e. medically assisted treatment).
- Provide long-term funding to secure naloxone availability for all Utahns. Consider the implementation of naloxone vending machines as a tool for easy distribution.
- Continue distributing FTS through local health departments and remove any local barriers which limit the distribution of FTS and other harm reduction resources.
- Provide a rapid, low-cost, publicly available drug checking program.
- Distribute excess naloxone kits to EMS so that responders can freely hand out extra kits on scene of an incident to others at high risk of experiencing or witnessing an overdose.
- Support community partners to provide more services that link clients to care (i.e. MAT Bridge programming) throughout the state.
- Prioritize ongoing Medicaid funding as a primary source for people seeking treatment.
- Expand definitions for grant funding to be used on indirect patient care (i.e. building expansion, offering longer clinical hours or providing room and board fees while in treatment).
- Provide grief and loss education in human services curricula, and offer no-cost continuing education units for current practitioners.
- Establish community advisory boards including people with lived experience to provide their input for policies and community interventions to reduce drug use and drug overdose events.
Recommendation 1: Public awareness campaigns
The 2021 Fentanyl Report stated the need for greater public awareness of the dangers of fentanyl based on numerous instances of young people experimenting with what they believed to be oxycodone tablets which were actually fentanyl tablets. Community outreach programs, such as syringe exchange services, emerged as a key strategic partner to amplify the harms of fentanyl. Since 2021, awareness of the presence of fentanyl has increased, and blue pills ("blues") made to look like pharmaceutical drugs are known to likely be fentanyl. The 2025 evaluation indicates that public awareness campaigns have progressed by 31%. Experts commented that "there was mainly only one campaign shared throughout Utah." Utah DHHS began the "Stop the Opidemic" campaign with a few sub-campaigns (i.e. "Know the Script," "Don't Use Alone"). Other campaigns (i.e. private campaigns) were not as far reaching or shared widely. At the time, there were campaigns that, though catchy and appealing for their ease, were most likely effective for adults but not adolescents. Recent studies show the negative impact of common messages similar to "One Pill Can Kill" or "Just Say NO." Fear-based approaches are less effective with youth due to several factors such as perceived unrealistic outcomes (18). Groups like the Utah National Guard have utilized more positive messaging especially among youth populations (i.e. "99% of your friends DON'T use drugs").

Local Efforts: Tri County Health Department notes using social media to spread awareness in addition to an informative podcast, radio ads, and information shared at events. They focus on sharing accurate information to counter misperceptions, especially in the tribal community. Utah County Health Department partners with local providers such as emergency departments and treatment facilities as well as law enforcement agencies to coordinate awareness and education efforts.
Recommendation 2: Naloxone distribution and availability
As fentanyl has become more prevalent in Utah, the need for greater access to naloxone has been highlighted. In fact, the recent decline in opioid overdose deaths in the United States has been credited to increased naloxone distribution. Even though naloxone administration is most effective in reversing an opioid overdose, challenges exist with its use and distribution:
- Facing stigma at pharmacies and potentially resulting in decreased distribution due to fear.
- More than one naloxone unit needed as an overdose may require more than one or two doses.
- Naloxone administration requires a second person who is sober and stable to administer the medication; however, PWUD more commonly overdose alone.
Since this recommendation was made in 2021, Utah has shown a 43% progression in the distribution and use of naloxone. This item was rated highest in the 2025 evaluation. Experts discussed the difficulty of purchasing naloxone by various agencies and advocacy groups based on prices as some groups can purchase naloxone less expensively than others. This impacts availability, especially in hard-to-reach and rural areas in Utah.
Naloxone vending machines are a tool that can be implemented to aid in widespread distribution. These machines, successfully implemented in Clark County, Nevada in 2019 (19), can be stocked to provide FTS, xylazine test strips, wound care kits and other harm reduction tools on top of naloxone. These machines can be accessed 24-hours and can easily be restocked to fit the needs of the population at hand.

Local Efforts: TriCounty health department routinely distributes naloxone and naloxone training in their area, in fact, four agencies in the area offer naloxone at no cost. In 2024, the TriCounty health department gave out over 500 naloxone kits and trained religious groups, local government, recreation districts, hotel staff, bar and club staff, school faculty, urgent care facilities, and general community members how to use it. They continue to collaborate with pharmacies to suggest naloxone when someone fills an opioid prescription, and offer information about where to obtain it for free including city offices, the Chamber of Commerce, and public libraries. In Utah County, efforts to increase distribution of naloxone include offering it to people leaving treatment, at medical visits, and for family/caregivers who attend appointments with high-risk individuals.
Recommendation 3: Access to fentanyl test strips and drug testing services
The Utah Department of Health and Human Services was first able to purchase fentanyl test strips (FTS) starting in 2023. In 2023, the Utah DHHS distributed about 2000 FTS to community partners for wider distribution. In 2024, this distribution grew to over 48,000. This information indicates that PWUD prefer to know the contents of their drug and to have a rapid and low cost way to test for possible contamination so that they can take the necessary precautions if fentanyl is present.
The 2021 FTS recommendation was rated at 29% progression. It is possible that the relevance of FTS is decreasing because fentanyl is assumed in nearly all drug products. Additionally, FTS only indicate the presence or absence of fentanyl but do not measure the potency of fentanyl present. For many PWUD who have encountered fentanyl, they are faced with the decision of continuing the use of their supply regardless of fentanyl presence. However, understanding the potency could provide more information to the PWUD as to what precautions they need to take. The evaluation highlighted the differences in FTS distribution across county lines. Although FTS has been removed from the drug paraphernalia list, some Utah local health departments have faced criticism or stigma on distributing FTS as well as other harm reduction resources and have opted not to distribute.

Local Efforts: TriCounty health department offers free fentanyl test strips and xylazine test strips (when available) through harm reduction services. TriCounty actively engages with their community to share when these test strips are available and any information about how to use them. Utah County Health Department has made its first FTS supply request from the state DHHS (May 2025). This request follows their efforts to demonstrate the necessity of FTS in their area.
Recommendation 4: Training and support for first responders
During the evaluation, experts discussed a constant need for first responder training, specifically in rural areas. Training has grown with many community partners as well as local health departments providing free or low cost opportunities. Experts discussed the potential to increase training to volunteer responders and to broaden contexts (i.e. schools). First responders from various fields participated in the evaluation and rated this recommendation at 21% progression.

Recommendation 5: Support for public health and public safety surveillance infrastructure
Experts reported a positive impact from collaboration between state agencies and crime labs on data sharing and resource allocation for harm reduction services. The Utah DHHS has implemented a SURE Plan in which drug event aberrations rapidly notify local health departments and community partners. This strategy combines surveillance systems in the emergency departments, the Office of the Medical Examiner's fatality dashboard and EMS reporting (through ODMAP). This extensive collaboration supports important public health warnings about drug supplies and drug events. However, respondents noted that more surveillance and training is needed with ample community partners involved. Experts acknowledge that implementation of these systems is slow and can be difficult to purchase. Improvement to public health and safety surveillance infrastructure was rated at 14% progression.

Local Efforts: The TriCounty Health Department refer to the ODMAP and Utah DHHS' SURE Plan to watch for trends in overdoses. The state has catered the dashboard to important local indicators.
Recommendation 6: Broaden overdose prevention programming to focus on all substances, not just opioids
The current phase of the drug epidemic the nation and Utah are facing is Wave IV which features fentanyl in most polysubstance supplies. Experts mention the rising toll of fentanyl on PWUD in Utah but discussed the need to continue focusing resources on all substances. While there isn't sufficient data to show a reduction in fentanyl use, increased awareness of lethal drug combinations could aid in reducing fatalities. This can be accomplished by providing FTS more readily and/or xylazine test strips as well as wound care kits to reduce harms from xylazine use. This recommendation was rated at 29% progression. Providing a range of resources in prevention and harm reduction efforts makes tackling all drug-related issues more effective.
Additionally, Utah has shown an increase in methamphetamine-related deaths year after year since 2020 (SUDORS data) and many experts acknowledge methamphetamine as the "silent killer." Broadening prevention efforts to help reduce all drug use and all drug overdose could curb overdose deaths in the future.

Local Efforts: While a lot of TriCounty area education is based on opioids, their training includes information on overdoses by non-opioid substances. Their Health Department offers Students Working Against Tobacco, a youth club with a focus on prevention of all substance misuse. Inpatient treatment centers in this area are not misuse specific with the exception of the detox center. The TriCounty Health Department's partners focus on all substance misuse in their public awareness campaigns.
Recommendation 7: Continued expansion of substance use disorder treatment options for all Utahns
In April 2021, the "X-waiver" was removed for clinicians to prescribe buprenorphine for treatment to those with opioid use disorder. This landmark success, along with expanding methadone fulfillment to four weeks rather than a daily dose and implementing more telemedicine options, gave those needing treatment more options. Though these programs have gained awareness in Utah, experts stress the need for continued support as PWUD rely heavily on them. Experts suggested expanding MAT Bridge programs where patients receive continued care from both pharmacological and behavioral treatment, noting this is the best-practice model.
Respondents mention the expensive cost of medications for opioid use disorder and Medicaid as a critical funding source. If Medicaid funds for Utahns are significantly reduced or lost all together, there would be a high potential of increased deaths related to drug use.
This recommendation was rated at 29% progression. Experts during the session commented on the need for clinics and servicers to use grant funding for often-overlooked services that are tangentially related to patient treatment. Such needs are expansion or maintenance of clinical buildings and widening clinic hours to evenings or late-shifts to broaden accessibility.

Local Efforts: TriCounty has a faith-based detox center for men, a tribal inpatient treatment center, and a treatment center for women under construction. This area has 10 providers offering medications for opioid use disorder and multiple mental health therapy options.
Recommendation 8: Grief and loss counseling and support groups
The loss of a loved one is complex and difficult, especially when sudden and traumatizing. Unresolved grief from a loss can lead to a higher risk of drug use and even drug overdose, among other ailments, making it important to offer support such as grief loss counseling. During this discussion, representatives of Utah's Caring Connections, a program from the University of Utah College of Nursing, shared the success of their program. Caring Connections is one of a handful of grief counseling programs offered throughout Utah. However, this recommendation was rated at 20% progression which could be due to the lack of trained professionals providing this type of support. Also, specialized support may be lacking rural areas due to travel distances.

Recommendation 9: Staff and equipment to the office of the medical examiner
This recommendation was rated at 17% progression. Though this score is fairly low, the recommendation was specific to the Office of the Medical Examiner and not generalizable to the evaluation respondents. However, experts mentioned the need to continuously support the Office of the Medical Examiner as this entity provides much needed toxicological data which assists in tracking consumption changes, impacts on demographics and monitoring drug use trends. As mentioned previously, the Office of the Medical Examiner also provides responses to understanding the scope of aberrations through the Utah DHHS SURE Plan initiative. Having historical data on drug use toxicology is paramount to understanding the scope of the aberration at hand.

Recommendation 10: Nothing about us, without us
It is largely recognized that involving those with lived experiences greatly benefits a program's success. Incorporating lived experience in programming helps those in treatment and recovery to make meaningful connections and be better informed potential outcomes. However, utilizing this science-based approach is more complex than simply inviting a lived experience perspective to the discussion. Experts in this evaluation reported the many attempts they had to include more lived experiences but many challenges were reported trying to facilitate this approach:
- Special permissions required to discuss these perspectives in schools and education centers
- Bias toward specific interventions is a potential as some out-of-recovery patients feel that their method is the only correct path,
- Compensation funding for those sharing their time and expertise.
Though this recommendation was rated at 24% progression, many experts reported the noticeable increase of incorporating people with lived experience in advisory positions for new policies and programs for PWUD. In fact, EMS responders mentioned the success of implementing a social worker response team for crisis intervention and representatives from recovery discussed integrating this method in peer recovery.

Local Efforts: The OFRC has recommended the use of peer-support services for those who have substance use disorders throughout the treatment process. Moreover, TriCounty has an LCSW that self-reports active recovery and promotes the benefits of others sharing their recovery journey.
References
- Park JN, et al., Situating the Continuum of Overdose Risk in the Social Determinants of Health: A New Conceptual Framework. Milbank Q, 2020. 98(3): p. 700-746
- Taylor, K., Singh, K., & Goyal, A. (2023, July). Fentanyl Transdermal. National Library of Medicine.
- Drugs of Abuse A DEA Resource Guide (2024 Edition). (2024). Drug Enforcement Administration, U.S. Department of Justice.
- U.S. Drug Enforcement Administration. (n.d.). Drug Scheduling.
- Han, Y., et al. (2019). The rising crisis of illicit fentanyl use, overdose, and potential therapeutic strategies. National Library of Medicine.
- Dahan, A., et al. (n.d.). Comparison of the respiratory effects of intravenous buprenorphine and fentanyl in humans and rats. British Journal of Anaesthesia.
- Schifano, F., et al. (2019). Assessing the 2004-2018 fentanyl misusing issues reported to an international range of adverse reporting systems. Frontiers in Pharmacology.
- Polysubstance overdose: Polysubstance overdose deaths have increased. (n.d.). CDC Overdose Prevention.
- Tanz, L., et al. (2024). Detection of illegally manufactured fentanyls and carfentanil in drug overdose deaths - United States, 2021-2024. CDC Morbidity and Mortality Weekly Report.
- Ciccarone, D., The Rise of Illicit Fentanyls, Stimulants and the Fourth Wave of the Opioid Overdose Crisis (2022). National Library of Medicine.
- Mars SG, Ondocsin J, and Ciccarone D, Sold as Heroin: Perceptions and Use of an Evolving Drug in Baltimore, MD. Journal of Psychoactive Drugs, 2018.
- Pardo, Bryce, et al. The Future of Fentanyl and Other Synthetic Opioids. Santa Monica, CA: RAND Corporation, 2019.
- Tamman, M., Gottesdiener, L., & Eisenhammer, S. (2024, July 25). FENTANYL EXPRESS | PART 1. Reuters.
- Jones CM, Einstein EB, Compton WM. Changes in synthetic opioid involvement in drug overdose deaths in the United States, 2010-2016. JAMA. 2018.
- DEA Emerging Threat Reports. (n.d.). In CESAR Center for Substance Use, Addiction & Health Research. University of Maryland.
- Cano M, Daniulaityte R, Marsiglia F. Xylazine in Overdose Deaths and Forensic Drug Reports in U.S. States, 2019-2022. JAMA 2024.
- CDC National Center for Health Statistics. (2025, May 14). Provisional Drug Overdose Death Counts. National Vital Statistics System.
- Hornik, R., et al. (2008). Effects of the National Youth Anti-Drug Media Campaign on Youths. American Journal of Public Health.
- Allen, S., et al. (2022). Evaluation the impact of naloxone dispensation at public health vending machines in Clark County, Nevada. Annals of Medicine.
Other sources:
- U.S. Department of Justice. (2025). 2025 National Drug Threat Assessment.
- Drug Seizure Statistics. (2025, May 12). U.S. Customs and Border Protection.
- Johnson, A. (2025). Utah Poison Control Center's 2024 Annual Report. U Health University of Utah.